In conversations across hospitals, one pattern kept surfacing repeatedly. Early discussions around capital equipment were usually optimistic. Clinical teams talked about better outcomes, faster workflows, improved precision, or stronger support during critical procedures. Interest was visible in the room. But the tone often shifted once the conversation moved beyond adoption and into ownership.
That change was subtle at first. Questions became slower, more operational, and far more cautious. People stopped talking only about what the equipment could do and started thinking about what would happen six months or three years later when the system became part of everyday hospital operations.
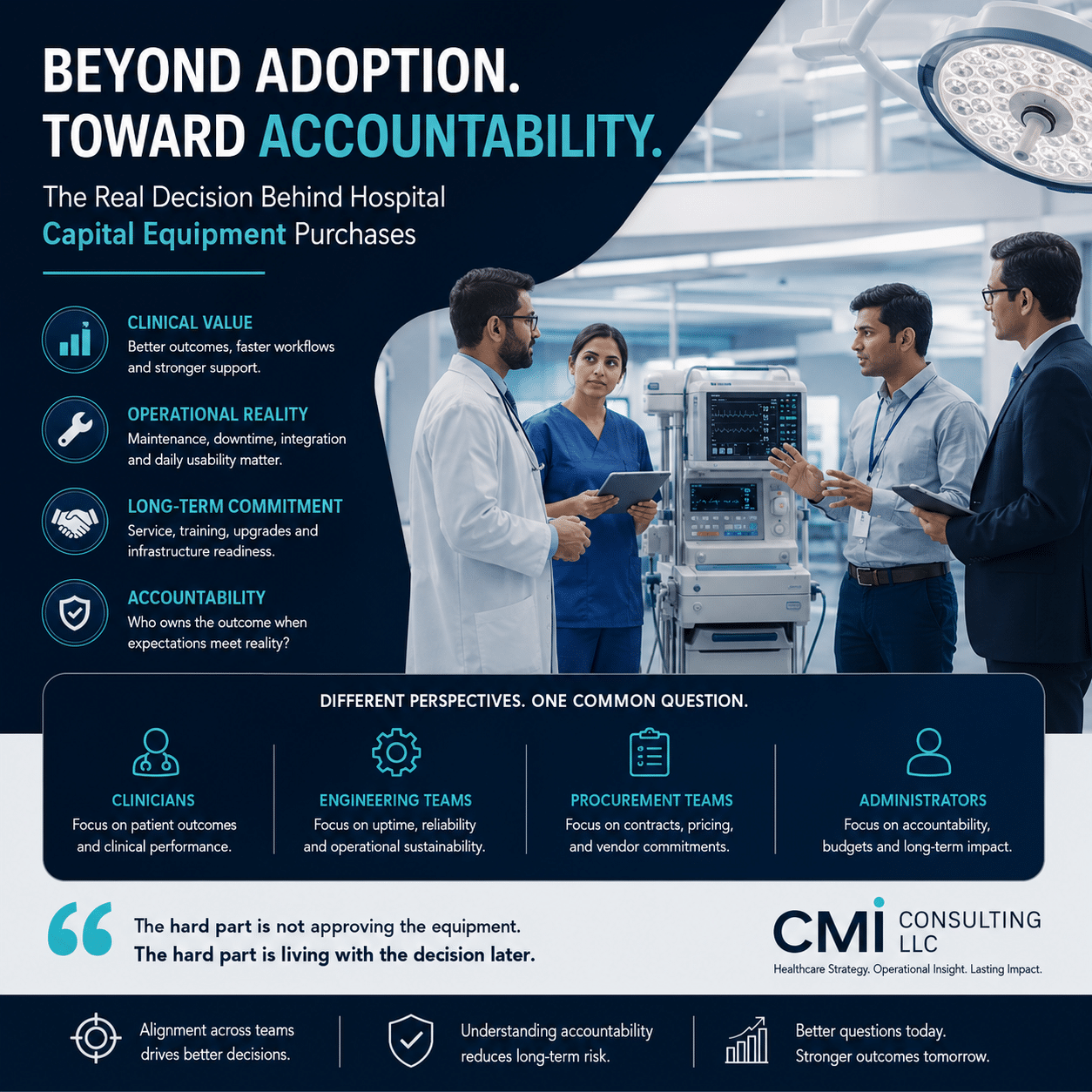
Across discussions with surgeons, intensivists, anesthesiologists, procurement teams, clinical engineering leaders, and hospital administrators, the same tension appeared in different forms. Excitement around capability was rarely the problem. The hesitation usually started when long-term accountability became harder to define.
Capital equipment decisions carry a different kind of weight inside hospitals. Unlike short-term purchases, these systems remain embedded in workflows for years. Once installed, they influence staffing, training, maintenance cycles, budgets, and patient care simultaneously. If things go smoothly, the equipment becomes invisible. If problems appear later, the visibility increases very quickly.
Several clinicians described situations where a device initially improved confidence during procedures but later created operational friction because servicing timelines, software integration, or maintenance realities were not fully understood upfront.
Clinical engineering teams often approached the same discussions from a completely different angle. Their concerns were less about first impressions and more about sustainability. Service responsiveness, downtime risk, compatibility with existing infrastructure, and internal maintenance pressure came up repeatedly.
Procurement and hospital administration teams viewed the conversation differently again.
Their focus naturally moved toward vendor commitments, long-term financial exposure, contract structures, and the possibility of being locked into support models that became difficult to manage later.
What stood out across all these conversations was not disagreement. Most groups generally understood the potential value of the equipment being discussed. The hesitation came from the fact that the long-term risks would not be experienced equally across teams.
Clinicians often carried the patient-facing responsibility. Engineering teams inherited operational pressure once systems entered regular use. Procurement teams remained accountable for vendor relationships, pricing structures, and service expectations over time. The further discussions moved into long-term operational reality, the more carefully decisions were approached.
Interestingly, very few people framed the issue as a lack of innovation or insufficient clinical value. In most cases, hospitals already understood the potential upside. The real uncertainty appeared around who would absorb the consequences if expectations and reality eventually separated.
One hospital administrator described it in a fairly direct way during a discussion:
“The hard part is not approving the equipment. The hard part is living with the decision later.” That feeling came up repeatedly in different ways. In practice, capital equipment adoption rarely slows because hospitals fail to see value. More often, momentum fades when accountability becomes fragmented and no single stakeholder fully owns the downside risk. That is usually the point where alignment becomes difficult.
Organizations involved in healthcare strategy and advisory work, including firms like CMI Consulting LLC, are increasingly seeing how these operational gaps influence purchasing behavior just as much as clinical evidence or pricing discussions.
Understanding how clinical teams, engineering leaders, and procurement stakeholders each define long-term responsibility often changes the direction of the conversation entirely. Because in hospital capital equipment decisions, the question is usually not whether the technology works.
The question is who remains accountable once the technology becomes part of everyday care.